
Blog

The medical billing process is one of the most critical functions for healthcare practices in Arizona, directly influencing cash flow and financial stability. For many providers, finding ways to improve the efficiency of their billing operations can lead to faster reimbursements, fewer errors, and better overall management of the practice.

Effective revenue cycle management (RCM) is essential for the success of any dermatology practice. From managing patient payments to ensuring timely insurance reimbursements, improving your RCM can directly impact your bottom line. Here are some practical tips to streamline your dermatology practice’s revenue cycle and maximize profitability. 1. Optimize Patient Scheduling and Registration An efficient scheduling and registration process is the foundation of a strong revenue cycle. Ensure that patient details, insurance information, and prior authorizations are verified during registration. This helps reduce claim denials and improves patient satisfaction. Tip: Automate appointment reminders and pre-registration forms to minimize errors and no-shows. 2. Invest in Dermatology-Specific Billing Software Using specialized billing software tailored for dermatology practices can streamline coding and claim submissions. These tools help ensure accurate documentation and improve compliance with the latest dermatology billing codes. Related: Learn how Medical Billing Companies Dermatology can provide tailored solutions to support your billing needs. 3. Train Staff on Coding and Documentation Proper coding and documentation are crucial for avoiding claim denials. Ensure your team is well-trained on dermatology-specific CPT and ICD-10 codes. Regular training sessions can keep your staff updated on new billing regulations and industry standards. Pro Tip: Collaborate with experts in Medical Billing Services Neurology for insights on handling complex coding scenarios. 4. Implement Regular Audits Conduct routine audits of your billing and coding processes to identify errors or inefficiencies. Audits can help pinpoint areas of improvement and ensure compliance with insurance requirements. 5. Monitor Key Performance Indicators (KPIs) Track KPIs such as claim denial rates, days in accounts receivable, and patient payment collection rates. Monitoring these metrics helps you identify trends and implement corrective actions promptly. 6. Enhance Patient Payment Collections Offer flexible payment options and ensure transparency in billing to improve patient collections. Clearly communicate payment expectations and provide multiple payment methods, such as online portals or mobile apps. Bonus: Practices offering Medical Billing Services Physical Therapy often use digital solutions for seamless payment collection—a strategy dermatology practices can adopt too. 7. Partner with a Professional Medical Billing Company Outsourcing your revenue cycle management to experts can free up valuable time and resources. Professional billing companies specialize in handling complex claims, reducing denials, and increasing revenue. Related: Discover how Medical Billing Companies Dermatology can transform your practice’s revenue cycle. Conclusion Improving your revenue cycle management is an ongoing process that requires attention to detail, regular updates, and a commitment to excellence. By optimizing scheduling, leveraging advanced technology, and partnering with experts, your dermatology practice can achieve financial stability and growth. Ready to take the next step? Explore how specialized medical billing services can revolutionize your practice today!
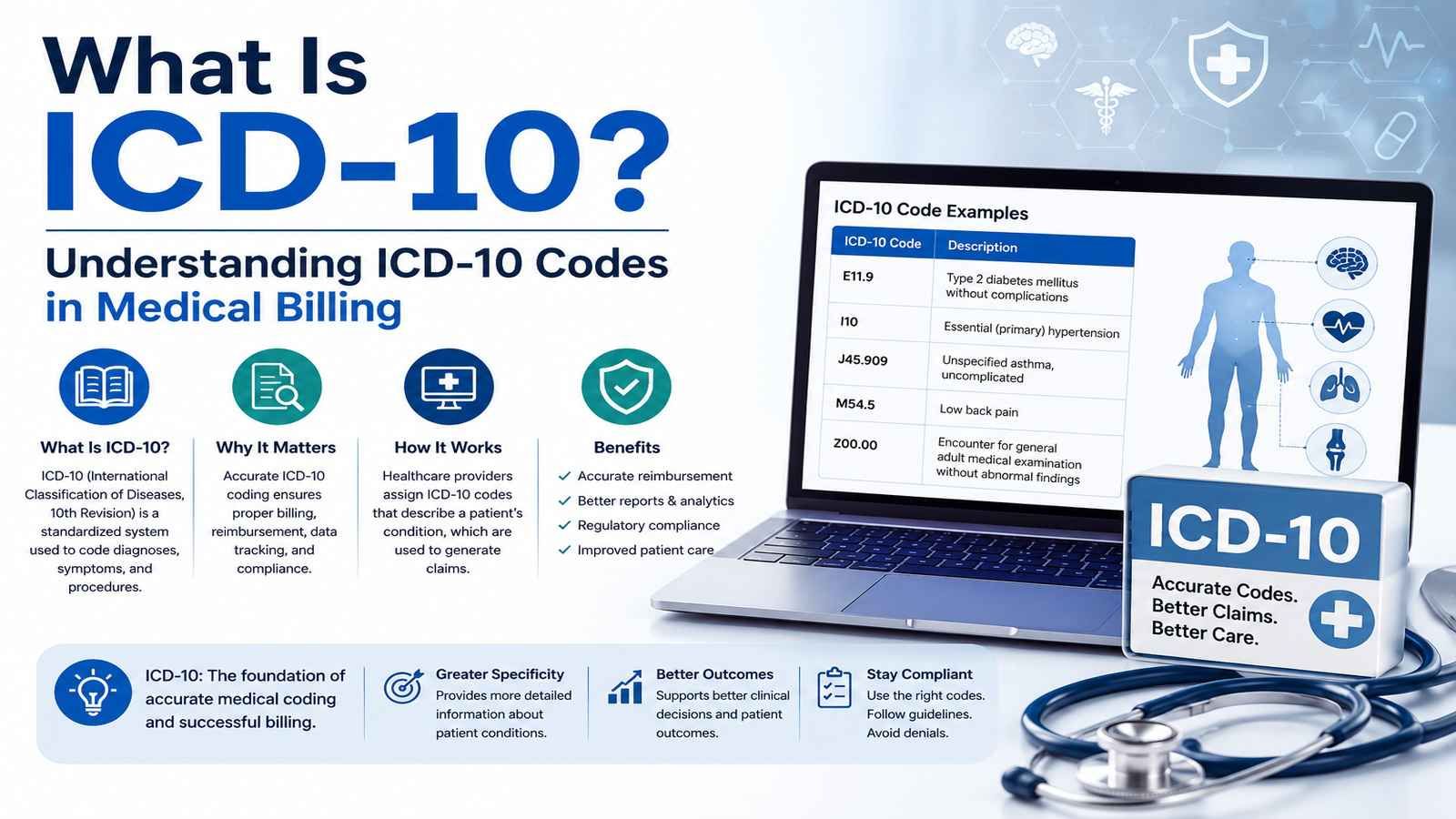
Learn what ICD-10 is, what ICD-10 codes mean, how they are used in medical billing, and the differences between ICD-9, ICD-10-CM, and ICD-10-PCS.
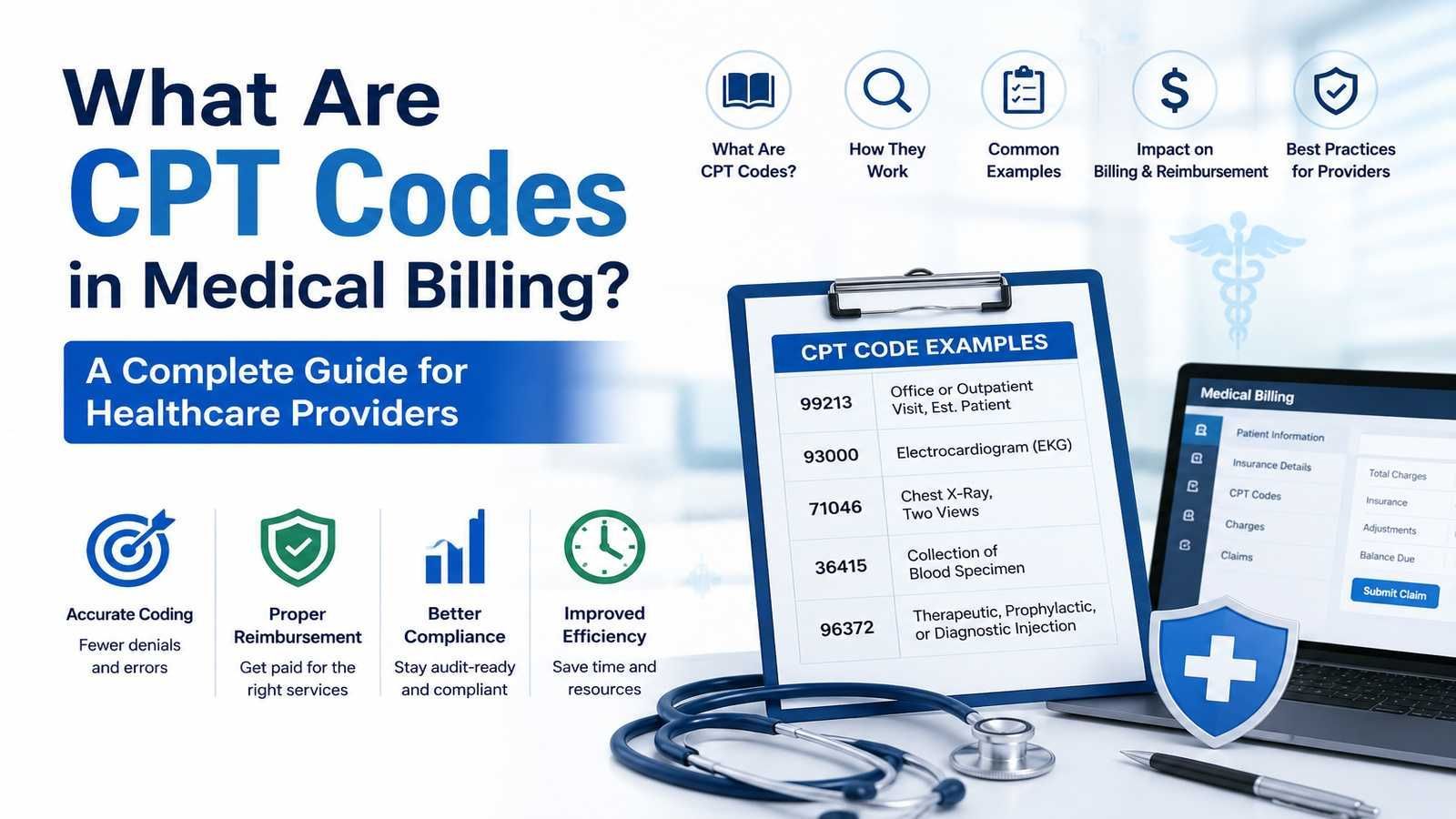
Accurate medical billing starts with accurate coding. One of the most important coding systems used in healthcare today is the CPT code system . Whether you're a physician, practice manager, or healthcare administrator, understanding CPT codes in medical billing is essential for reducing claim denials, improving reimbursement rates, and maintaining compliance. Every year, millions of insurance claims are processed using CPT codes. These standardized codes help insurance companies understand what services were provided, determine reimbursement eligibility, and process claims efficiently. At Valley Medical Billing , proper CPT coding is a critical part of helping healthcare practices maximize revenue and avoid costly billing errors. What Is a CPT Code? CPT stands for Current Procedural Terminology. Developed and maintained by the American Medical Association (AMA) , CPT codes are five-character codes used to describe medical, surgical, diagnostic, and evaluation services performed by healthcare providers. In simple terms, a CPT code tells an insurance company: What service was provided Who provided the service When the service occurred How the provider should be reimbursed Without proper CPT coding, healthcare providers may experience claim denials, underpayments, or payment delays. What Are CPT Codes Used For? CPT codes are used throughout the healthcare revenue cycle. They help with: Insurance Claims Processing Insurance companies use CPT codes to determine coverage and reimbursement amounts. Medical Billing Billing teams include CPT codes on claims submitted to commercial insurers, Medicare, and Medicaid. Revenue Cycle Management Accurate CPT coding supports clean claim submissions and improves reimbursement performance. Healthcare Reporting Providers and healthcare organizations use coding data for quality reporting, utilization tracking, and compliance purposes. How CPT Coding Works in Medical Billing When a patient receives medical care, the provider documents the visit in the patient's chart or EHR system. Certified coders then review the documentation and assign the appropriate CPT code based on the services performed. The billing workflow generally follows these steps: Patient receives treatment Provider documents the encounter CPT and diagnosis codes are assigned Claim is submitted to the payer Insurance reviews the claim Reimbursement is issued or additional information is requested Even small coding errors can result in claim rejections, making CPT coding one of the most important parts of medical billing. Types of CPT Codes Many providers ask, "What are the three categories of CPT codes?" The CPT code system is divided into three primary categories. Category I CPT Codes These are the most commonly used CPT codes in healthcare. They cover: Office visits Surgical procedures Radiology services Laboratory testing Pathology services Anesthesia services Examples include: 99213 – Established patient office visit 99214 – Moderate complexity office visit 93000 – Electrocardiogram (EKG) Category II CPT Codes Category II codes are used for performance measurement and quality reporting. These codes help healthcare organizations track outcomes and compliance with quality initiatives. Unlike Category I codes, they are generally not used for reimbursement. Category III CPT Codes Category III codes are temporary codes assigned to emerging technologies, procedures, and services. These codes allow healthcare organizations to track new treatments before permanent CPT codes are created. CPT Codes vs ICD-10 Codes: What's the Difference? Many healthcare professionals confuse CPT and ICD-10 codes. Here's a simple distinction: CPT Codes Describe what service or procedure was performed . ICD-10 Codes Describe why the service was performed by identifying the patient's diagnosis or condition. For example: ICD-10 Code J02.9 – Acute pharyngitis CPT Code 99213 – Office visit Both codes work together to support medical necessity and insurance reimbursement. Common CPT Code Examples Understanding common CPT code examples can help providers better understand claim submissions. CPT Code Description 99213 Established patient office visit 99214 Moderate complexity office visit 90686 Influenza vaccine administration 93000 Electrocardiogram (EKG) 71046 Chest X-ray, two views The exact reimbursement associated with a CPT code depends on payer contracts, geographic location, and insurance policies. Common CPT Coding Mistakes That Cause Claim Denials Incorrect CPT coding is one of the leading causes of denied medical claims. Common errors include: Upcoding Billing for a higher-level service than documented. Undercoding Billing for a lower-level service than performed. Missing Modifiers Failing to include necessary CPT modifiers when required. Documentation Gaps Insufficient clinical documentation to support the reported service. Outdated CPT Codes Using retired or revised codes that are no longer accepted. Regular coding audits and professional billing support can significantly reduce these issues. How CPT Codes Impact Reimbursement Insurance companies rely heavily on CPT codes when calculating payments. Incorrect coding can lead to: Reduced reimbursement Claim denials Payment delays Compliance risks Audit exposure That's why accurate CPT coding in medical billing is essential for maintaining a healthy revenue cycle. Practices that invest in proper coding processes often experience improved collections and fewer billing issues. How Valley Medical Billing Helps Healthcare Providers At Valley Medical Billing , accurate coding is a core component of our revenue cycle management services. Our team helps healthcare providers: Assign accurate CPT codes Reduce coding-related claim denials Improve reimbursement accuracy Stay compliant with payer requirements Optimize medical billing workflows By combining coding expertise with proactive claim management, we help healthcare practices strengthen their financial performance. FAQs What does CPT stand for in medical billing? CPT stands for Current Procedural Terminology , a coding system developed by the American Medical Association (AMA) to describe medical procedures and services. What are CPT codes used for? CPT codes are used to report medical procedures and services for insurance claims, billing, reimbursement, and healthcare reporting. What are the three categories of CPT codes? The three main CPT code categories are: Category I (standard procedures and services) Category II (performance measurement) Category III (emerging technologies) What is the difference between CPT and ICD-10 codes? CPT codes describe the service performed, while ICD-10 codes describe the patient's diagnosis or condition. Why are CPT codes important in medical billing? CPT codes determine how services are reported to insurance companies and directly affect claim approval and reimbursement amounts.
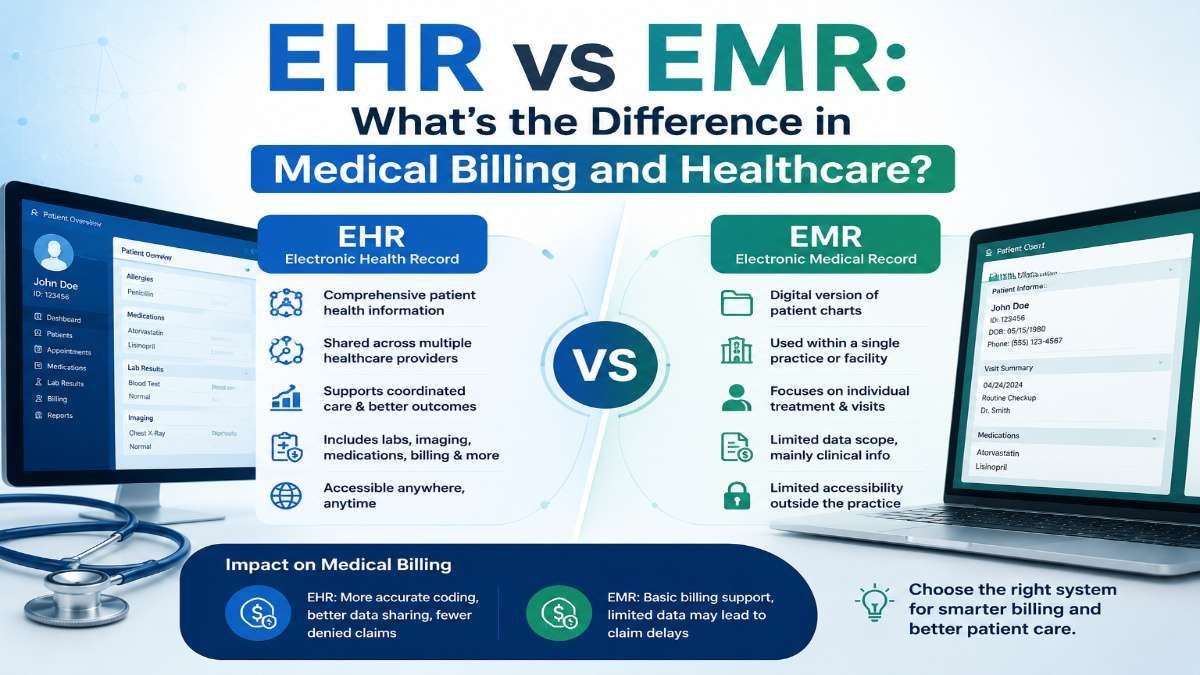
Learn the difference between EHR vs EMR, how electronic medical records impact medical billing, and why accurate documentation matters for healthcare providers.
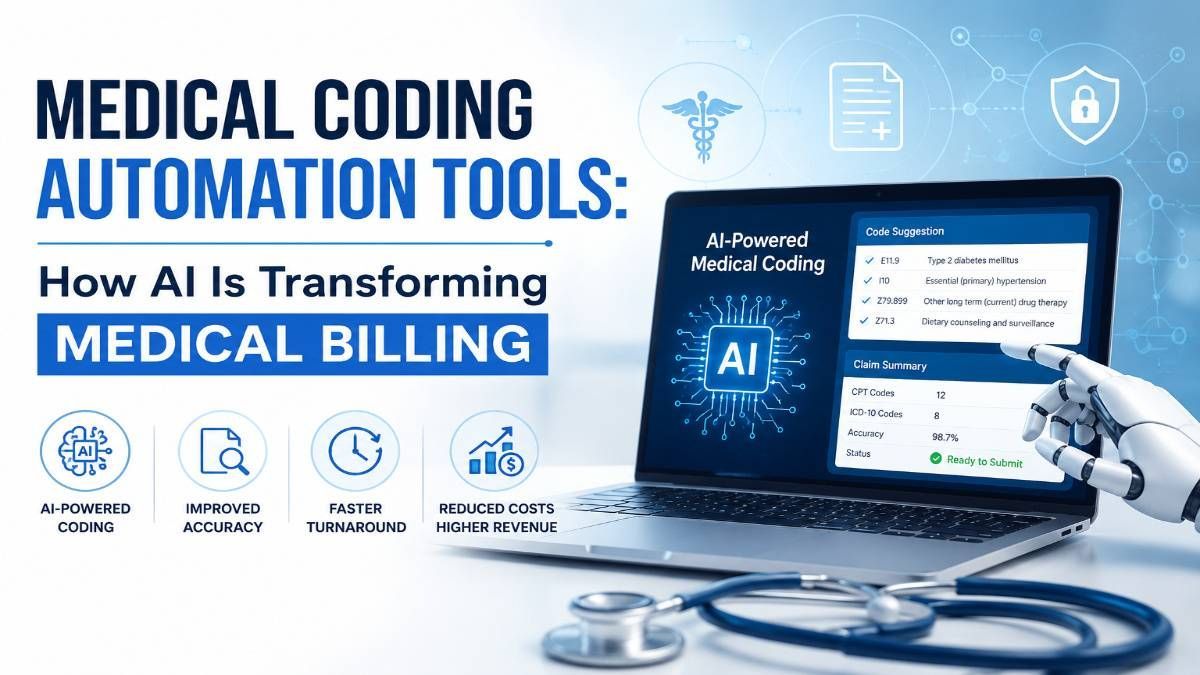
Learn how medical coding automation tools improve accuracy, reduce claim denials, and streamline revenue cycle management for healthcare providers.
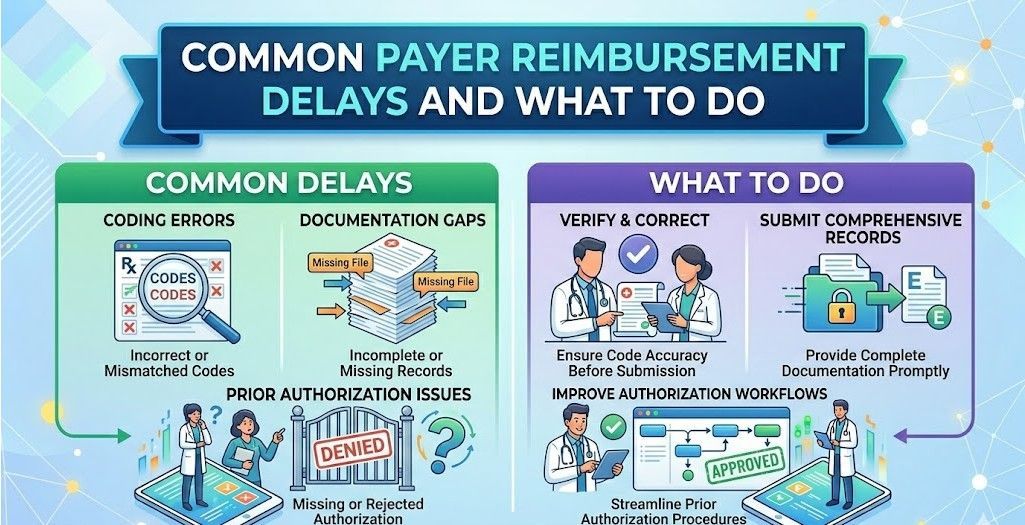
Delayed insurance payments are one of the most common reasons medical practices experience cash flow stress. Even when claims are submitted correctly, reimbursement can stall for weeks or months due to payer processing issues, credentialing gaps, or administrative errors. Understanding why reimbursement delays happen and how to respond proactively helps practices reduce aging accounts receivable and maintain financial stability. Why Payer Reimbursement Delays Hurt Practice Revenue Reimbursement delays affect more than just cash flow. They increase administrative workload, slow down growth, and often lead to missed appeal deadlines. Common consequences include: Rising accounts receivable over 60 and 90 days Staff time wasted on payer follow ups Difficulty forecasting monthly revenue Increased risk of claim write offs Most delays are preventable once their root cause is identified. Common Causes of Payer Reimbursement Delays Identifying the source of delay is the first step toward faster payment. Incomplete or Incorrect Claim Information Missing demographics, incorrect policy numbers, or coding inconsistencies can place claims into manual review queues. These claims often remain unpaid until corrections are made. Credentialing and Enrollment Issues If a provider is not properly credentialed or enrolled with the payer, claims may be held or denied. Even small enrollment mismatches can result in payment delays. Prior Authorization Problems Claims submitted without valid prior authorization often require additional review. Some payers delay payment even when authorization exists but is not linked correctly. Coordination of Benefits Conflicts When patients have multiple insurance plans, payers may delay processing until coverage order is confirmed. COB issues frequently cause payment stagnation. Payer Backlogs and Policy Changes Payers may experience internal backlogs or change coverage policies without timely notification. These delays affect large volumes of claims simultaneously. How to Identify Reimbursement Delays Early Early detection prevents claims from aging unnecessarily. Monitor Aging Reports Weekly Review claims approaching 30 and 45 days. Early intervention reduces the risk of extended delays. Track Payer Specific Patterns If one payer consistently delays payments, there may be systemic issues related to credentialing, documentation, or submission format. Flag Claims Pending Medical Review Claims in medical review status should be monitored closely and followed up on regularly. What to Do When Payer Payments Are Delayed A structured response helps recover revenue faster. Verify Claim Acceptance Confirm that the payer accepted the claim and did not reject it at the clearinghouse level. Check Provider Credentialing Status Ensure the rendering and billing providers are fully credentialed and enrolled with the payer. Credentialing gaps are one of the most overlooked causes of delayed reimbursement. Contact the Payer Strategically Follow payer specific timelines for follow up. Document reference numbers, call dates, and outcomes for every interaction. Submit Supporting Documentation Promptly If the payer requests additional records, submit them immediately to avoid further delay. Escalate When Necessary Claims that exceed payer processing timelines should be escalated through formal inquiries or appeals. Preventing Future Reimbursement Delays Prevention reduces dependency on follow ups and appeals. Verify patient eligibility and coverage at every visit Maintain up to date provider credentialing records Track authorization requirements by payer Submit clean claims with complete documentation Audit denial and delay trends monthly Proactive workflows improve reimbursement speed and reduce operational strain. FAQs on Payer Reimbursement Delays How long should payer reimbursement normally take? Most payers process clean claims within 15 to 30 days. Claims exceeding this range require follow up. Can credentialing issues delay payment even if the claim is accepted? Yes. Claims may be accepted but placed on hold until credentialing or enrollment is resolved. Should delayed claims be appealed? Appeals are appropriate when payer processing timelines are exceeded or when delays turn into denials. How often should billing teams follow up on delayed claims? Follow up every 15 to 20 days, depending on payer guidelines. Do payer delays impact patient billing? Yes. Delays can affect patient statements and increase confusion around balances. Valley Medical Billing Support for Faster Reimbursement Reducing reimbursement delays requires strong billing workflows and accurate provider enrollment. Valley Medical Billing helps practices identify payer bottlenecks, resolve credentialing issues, and streamline follow up processes. If provider enrollment or payer participation is slowing down your payments, our team works closely with practices seeking reliable Medical Credentialing Services Near Me to ensure providers are properly enrolled and claims are reimbursed without unnecessary delays.
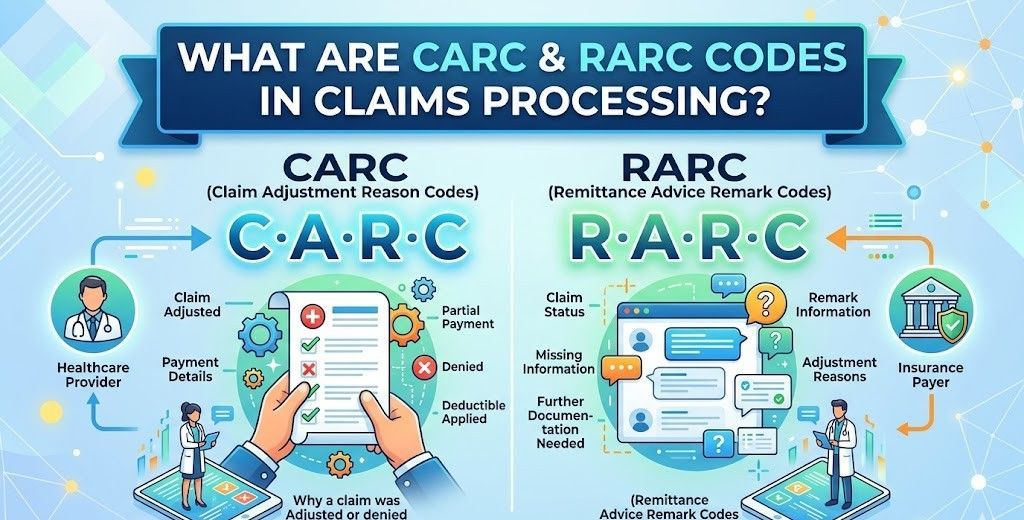
Unclear denial messages are one of the most frustrating issues in medical billing. When a claim is denied without a clear explanation, billing teams waste time guessing, resubmitting incorrectly, or delaying follow up. This confusion often leads to lost revenue. CARC and R ARC codes exist to solve this problem. Understanding these codes allows practices to identify denial reasons quickly and take the right corrective action the first time. Understanding CARC Codes in Medical Billing CARC stands for Claim Adjustment Reason Code. These codes explain why a claim or service line was reduced, adjusted, or denied by the payer. Every remittance advice includes at least one CARC code when payment is not made in full. What CARC Codes Indicate CARC codes typically point to issues such as: • Missing or incorrect patient information • Coverage or eligibility problems • Coding or modifier errors • Authorization or referral issues • Timely filing limits • Duplicate billing Because CARC codes directly affect payment, they are the starting point for denial analysis. Common CARC Code Examples Some frequently seen CARC codes include: • CARC 16 for missing or incomplete information • CARC 18 for duplicate claim or service • CARC 50 for non covered services • CARC 197 for missing prior authorization Each code highlights what triggered the adjustment so billers know where to investigate. Understanding RARC Codes for Denial Clarification RARC stands for Remittance Advice Remark Code. These codes provide additional details that explain or expand on the CARC code. If CARC codes explain the reason for the denial, RARC codes explain what needs to be fixed. What RARC Codes Tell You RARC codes may indicate: • Which documentation is missing • Where to submit additional information • Why a policy requirement was not met • Which payer rule applies to the claim RARC codes guide billers toward the correct correction instead of guessing. Common RARC Code Examples Examples include: • N290 for missing referral or authorization number • M124 for missing clinical or operative notes • N130 instructing review of payer policy • N780 for missing or invalid provider taxonomy Together, CARC and RARC codes give a complete explanation for claim adjustment. Why CARC and RARC Codes Matter in Claims Processing Practices that understand these codes resolve denials faster and reduce rework. Clear interpretation leads to: 1. Faster identification of denial root causes 2. More accurate claim corrections 3. Fewer repeated denials 4. Improved cash flow 5. Reduced staff frustration Ignoring or misunderstanding these codes often results in avoidable write offs. Common Mistakes When Handling CARC and RARC Codes Many billing teams struggle with denial resolution due to: • Correcting the wrong issue • Resubmitting claims without reviewing RARC details • Missing appeal deadlines • Failing to track recurring denial patterns These mistakes slow down reimbursement and create unnecessary backlogs. Best Practices for Responding to CARC and RARC Codes Following a structured approach improves denial outcomes. Review Both Codes Together Always analyze the CARC and RARC codes as a pair. One explains the denial, the other explains the fix. Validate Against Payer Policy Confirm the denial is valid. Some denials occur due to outdated eligibility or payer system errors. Correct and Resubmit Promptly Timely filing rules still apply after denial. Fast action prevents permanent revenue loss. Track Denial Trends Recurring codes usually point to workflow issues such as registration errors or coding gaps. Train Billing Staff Regularly CARC and RARC codes are updated quarterly. Regular training keeps teams compliant and efficient. FAQs About CARC and RARC Codes Are CARC and RARC codes standardized across payers? Yes, most are standardized, but some payers include additional proprietary remark codes. Can a claim have multiple CARC or RARC codes? Yes, a single claim can include multiple codes depending on the issues identified. Are CARC and RARC codes appealable? Yes, if documentation supports the claim, denials associated with these codes can be appealed. How often are CARC and RARC codes updated? They are updated quarterly, and billing teams should review updates regularly. What happens if RARC codes are ignored? Ignoring RARC codes often leads to repeated denials because the underlying issue was never corrected. Valley Medical Billing Support for Denial Management Accurately interpreting CARC and RARC codes is essential for protecting revenue. If your practice is struggling with denial resolution, working with experienced professionals can make a measurable difference. Valley Medical Billing collaborates with trusted Medical Billing Companies Nevada to help practices improve claims processing, reduce denials, and recover revenue faster through structured denial management and payer follow up.

In the world of medical billing, accuracy is everything. One of the most serious issues practices face is upcoding—the act of billing for a higher-level service than what was actually provided. While sometimes intentional, upcoding often happens by mistake, leaving providers exposed to audits, penalties, and even fraud allegations. For healthcare practices, understanding what upcoding is and how to prevent it is critical to maintaining compliance and financial stability. What Is Upcoding in Medical Billing? Upcoding occurs when a provider bills insurance for a service at a higher reimbursement rate than what was delivered. This usually happens by: • Assigning a more complex CPT code than the documentation supports • Submitting claims for services that were more intensive or time-consuming than actually provided • Using modifiers incorrectly to inflate reimbursement Example: A provider bills for a 60-minute patient evaluation (99215) when the visit lasted only 25 minutes (99213). Why Upcoding Is a Serious Compliance Risk Upcoding isn’t just a billing error—it can be viewed as fraud under federal law. The risks include: • Legal exposure: Practices may face lawsuits under the False Claims Act. • Financial penalties: Fines can reach up to three times the overbilled amount. • Loss of reputation: Investigations damage patient trust and payer relationships. • Audit risk: Payers and government agencies closely monitor coding patterns. Even if upcoding is unintentional, regulators may still treat it as fraudulent activity. Common Causes of Unintentional Upcoding Many practices don’t set out to commit fraud. Instead, errors usually happen due to: • Insufficient documentation – Notes don’t match the level of service billed. • Complex coding guidelines – Providers and staff may struggle with evolving CPT/ICD-10 rules. • Over-reliance on EHR templates – Automated code suggestions may default to higher levels of service. • Lack of training – Staff unaware of compliance standards can make mistakes. How to Prevent Upcoding in Your Practice To protect your practice from legal and financial consequences: • Ensure accurate documentation: Providers must record details that justify the billed service. • Invest in staff training: Ongoing coding and compliance education reduces errors. • Perform regular audits: Internal reviews catch mistakes before payers do. • Leverage credentialing support: Working with experts in Medical Credentialing California helps ensure providers are properly authorized and follow payer requirements. • Use compliance software: Tools with claim scrubbing and coding checks minimize risks. Legal Exposure Due to Unintentional Fraud The biggest fear for many practices is being accused of fraud when mistakes were simply unintentional. Upcoding—even when accidental—can trigger costly investigations. By taking proactive steps to ensure compliance, providers reduce their legal exposure while protecting revenue streams. FAQs About Upcoding in Medical Billing 1. What’s the difference between upcoding and unbundling? • Upcoding bills for a higher-level service than provided. • Unbundling splits services that should be billed together. Both are considered compliance risks. 2. Can upcoding happen accidentally? Yes. Many cases occur due to documentation gaps, coding complexity, or EHR errors rather than intentional fraud. 3. Who investigates upcoding cases? Medicare, Medicaid, private insurers, and the Office of Inspector General (OIG) may all audit claims for upcoding. 4. How can practices protect themselves from upcoding audits? Conduct regular internal audits, train staff on coding accuracy, and ensure documentation fully supports billed services. Final Thoughts Upcoding may seem like a small error, but its consequences are significant. Whether accidental or intentional, it exposes providers to legal, financial, and reputational risks. By prioritizing accurate documentation, regular compliance checks, and proper credentialing, practices can protect themselves and build long-term trust with payers and patients alike.

Choosing professional Medical Billing Services in Arizona offers healthcare providers numerous advantages. Whether you're running a small clinic or a larger healthcare facility, in-house billing can be overwhelming and prone to errors.